The paper as published -I have altered nothing
Click to access Hydroxychloroquine_final_DOI_IJAA.pdf
Here we go – just in case it disapears like so many things have
I try to do things in triplicate —-AT LEAST
Abstract
Background
Chloroquine and hydroxychloroquine have been found to be efficient on SARS-CoV-2, and
reported to be efficient in Chinese COV-19 patients. We evaluate the role of
hydroxychloroquine on respiratory viral loads.
Patients and methods
French Confirmed COVID-19 patients were included in a single arm protocol from early
March to March 16th
, to receive 600mg of hydroxychloroquine daily and their viral load in
nasopharyngeal swabs was tested daily in a hospital setting. Depending on their clinical
presentation, azithromycin was added to the treatment. Untreated patients from another center
and cases refusing the protocol were included as negative controls. Presence and absence of
virus at Day6-post inclusion was considered the end point.
Results
Six patients were asymptomatic, 22 had upper respiratory tract infection symptoms and eight
had lower respiratory tract infection symptoms.
Twenty cases were treated in this study and showed a significant reduction of the viral
carriage at D6-post inclusion compared to controls, and much lower average carrying duration
than reported of untreated patients in the literature. Azithromycin added to
hydroxychloroquine was significantly more efficient for virus elimination.
Conclusion
Despite its small sample size our survey shows that hydroxychloroquine treatment is
significantly associated with viral load reduction/disappearance in COVID-19 patients and its
effect is reinforced by azithromycin.
Key words: 2019-nCoV; SARS-CoV-2; COVID-19; hydroxychloroquine; azithomycin;
clinical trial
1. Introduction
In late December 2019, an outbreak of an emerging disease (COVID-19) due to a novel
coronavirus (named SARS-CoV-2 latter) started in Wuhan, China and rapidly spread in China
and outside [1,2]. The WHO declared the epidemic of COVID-19 as a pandemic on March
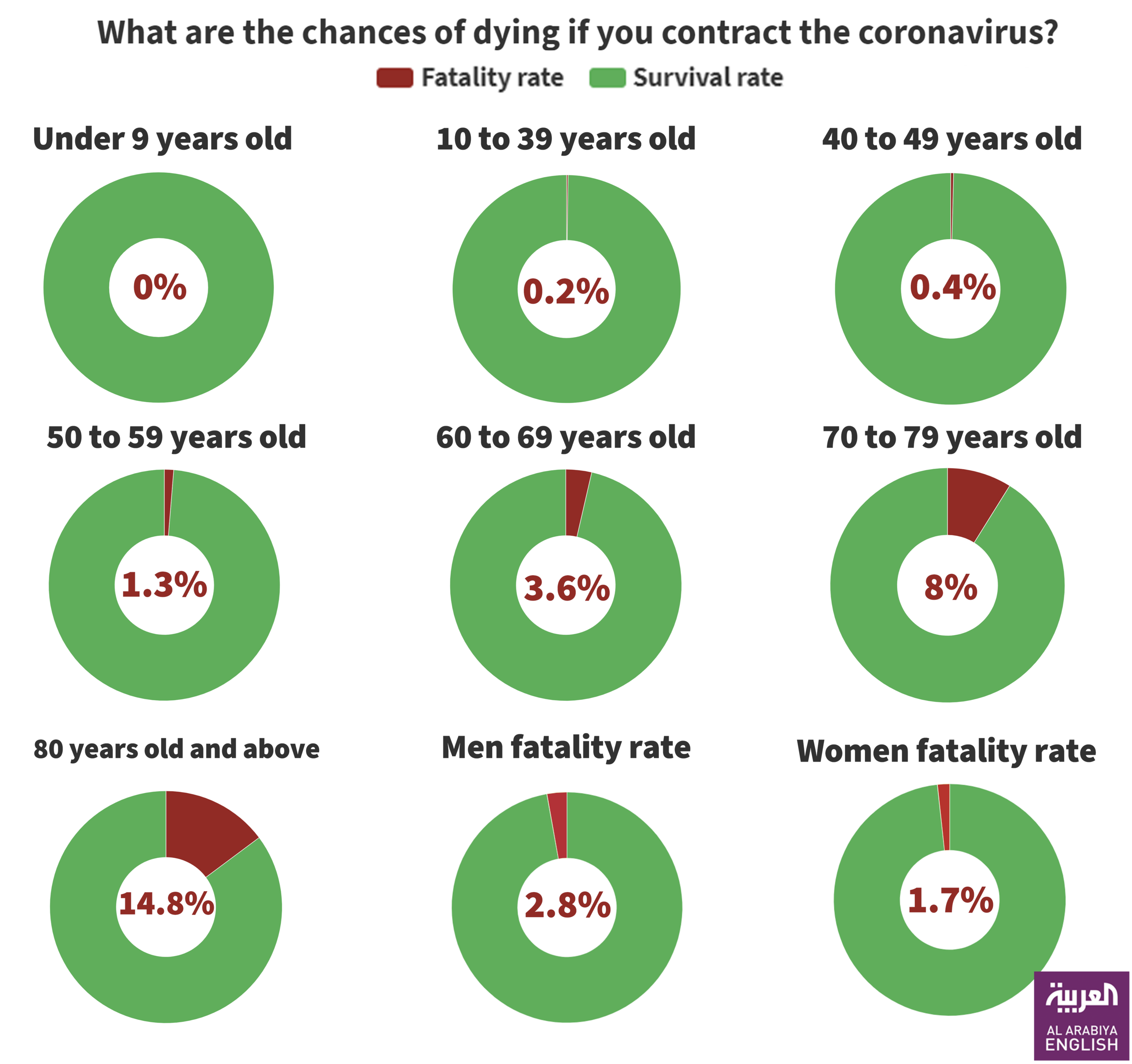
12th 2020 [3]. According to a recent Chinese stud, about 80% of patients present with mild
disease and the overall case-fatality rate is about 2.3% but reaches 8.0% in patients aged 70 to
79 years and 14.8% in those aged >80 years [4]. However, there is probably an important
number of asymptomatic carriers in the population, and thus the mortality rate is probably
overestimated. France is now facing the COVID-19 wave with more than 4500 cases, as of
March 14th 2020 [5]. Thus, there is an urgent need for an effective treatment to treat
symptomatic patients but also to decrease the duration of virus carriage in order to limit the
transmission in the community. Among candidate drugs to treat COVID-19, repositioning of
old drugs for use as antiviral treatment is an interesting strategy because knowledge on safety
profile, side effects, posology and drug interactions are well known [6,7].
A recent paper reported an inhibitor effect of remdesivir (a new antiviral drug) and
chloroquine (an old antimalarial drug) on the growth of SARS-CoV-2 in vitro, [8] and an
early clinical trial conducted in COVID-19 Chinese patients, showed that chloroquine had a
significant effect, both in terms of clinical outcome and viral clearance, when comparing to
controls groups [9,10]. Chinese experts recommend that patients diagnosed as mild, moderate
and severe cases of COVID-19 pneumonia and without contraindications to chloroquine, be
treated with 500 mg chloroquine twice a day for ten days [11].
Hydroxychloroquine (an analogue of chloroquine) has been demonstrated to have an anti-
SARS-CoV activity in vitro [12]. Hydroxychloroquine clinical safety profile is better than that
of chloroquine (during long-term use) and allows higher daily dose [13] and has fewer
6
concerns about drug-drug interactions [14]. Our team has a very comprehensive experience in
successfully treating patients with chronic diseases due to intracellular bacteria (Q fever due
to Coxiella burnetii and Whipple’s disease due to Tropheryma whipplei) with long-term
hydroxychloroquine treatment (600 mg/day for 12 to 18 months) since more than 20 years.
[15,16] We therefore started to conduct a clinical trial aiming at assessing the effect of
hydroxychloroquine on SARS-CoV-2-infected patients after approval by the French Ministry
of Health. In this report we describe our early results, focusing on virological data in patients
receiving hydroxychloroquine as compared to a control group.
2. Study population and Methods
Setting
This ongoing study is coordinated by The Méditerranée Infection University Hospital Institute
in Marseille. Patients who were proposed a treatment with hydroxychloroquine were recruited
and managed in Marseille centre. Controls without hydroxychloroquine treatment were
recruited in Marseille, Nice, Avignon and Briançon centers, all located in South France.
Patients
Hospitalized patients with confirmed COVID-19 were included in this study if they fulfilled
two primary criteria: i) age >12 years; ii) PCR documented SARS-CoV-2 carriage in
nasopharyngeal sample at admission whatever their clinical status.
Patients were excluded if they had a known allergy to hydroxychloroquine or chloroquine or
had another known contraindication to treatment with the study drug, including retinopathy,
G6PD deficiency and QT prolongation. Breastfeeding and pregnant patients were excluded
based on their declaration and pregnancy test results when required.
7
Informed consent
Before being included in the study, patients meeting inclusion criteria had to give their
consent to participate to the study. Written informed signed consent was obtained from adult
participants (> 18 years) or from parents or legal guardians for minors (<18 years). An
information document that clearly indicates the risks and the benefits associated with the
participation to the study was given to each patient. Patients received information about their
clinical status during care regardless of whether they participate in the study or not. Regarding
patient identification, a study number was assigned sequentially to included participants,
according to the range of patient numbers allocated to each study centre. The study was
conducted in accordance with the International Council for Harmonisation of Technical
Requirements for Pharmaceuticals for Human Use (ICH) guidelines of good clinical practice,
the Helsinki Declaration, and applicable standard operating procedures.
The protocol, appendices and any other relevant documentation were submitted to the French
National Agency for Drug Safety (ANSM) (2020-000890-25) and to the French Ethic
Committee (CPP Ile de France) (20.02.28.99113) for reviewing and approved on 5th and 6th
March, 2020, respectively. This trial is registered with EU Clinical Trials Register, number
2020-000890-25.
Procedure
Patients were seen at baseline for enrolment, initial data collection and treatment at day-0, and
again for daily follow-up during 14 days. Each day, patients received a standardized clinical
examination and when possible, a nasopharyngeal sample was collected. All clinical data
were collected using standardized questionnaires. All patients in Marseille center were
proposed oral hydroxychloroquine sulfate 200 mg, three times per day during ten days (in this
preliminary phase ,we did not enrolled children in the treatment group based in data indicating
that children develop mild symptoms of COVID-19 [4]). Patients who refused the treatment
8
or had an exclusion criteria, served as controls in Marseille centre. Patients in other centers
did not receive hydroxychloroquine and served as controls. Symptomatic treatment and
antibiotics as a measure to prevent bacterial super-infection was provided by investigators
based on clinical judgment. Hydroxychloroquine was provided by the National Pharmacy of
France on nominative demand.
Clinical classification
Patients were grouped into three categories: asymptomatic, upper respiratory tract infection
(URTI) when presenting with rhinitis, pharyngitis, or isolated low-grade fever and myalgia,
and lower respiratory tract infections (LRTI) when presenting with symptoms of pneumonia
or bronchitis.
PCR assay
SARS-CoV-2 RNA was assessed by real-time reverse transcription-PCR [17].
Hydroxychloroquine dosage
Native hydroxychloroquine has been dosed from patients’ serum samples by UHPLC-UV
using a previously described protocol [18]. The peak of the chromatogram at 1.05 min of
retention corresponds to hydroxychloroquine metabolite. The serum concentration of this
metabolite is deduced from UV absorption, as for hydroxychloroquine concentration.
Considering both concentrations provides an estimation of initial serum hydroxychloroquine
concentration.
Culture
9
For all patients, 500 μL of the liquid collected from the nasopharyngeal swab were passed
through 0.22-μm pore sized centrifugal filter (Merck millipore, Darmstadt, Germany), then
were inoculated in wells of 96-well culture microplates, of which 4 wells contained Vero E6
cells (ATCC CRL-1586) in Minimum Essential Medium culture medium with 4% fetal calf
serum and 1% glutamine. After centrifigation at 4,000 g, microplates were incubated at 37°C.
Plates were observed daily for evidence of cytopathogenic effect. Presumptive detection of
virus in supernatant was done using SU5000 SEM (Hitachi) then confirmed by specific RT-
PCR.
Outcome
The primary endpoint was virological clearance at day-6 post-inclusion. Secondary outcomes
were virological clearance overtime during the study period, clinical follow-up (body
temperature, respiratory rate, long of stay at hospital and mortality), and occurrence of side-
effects.
Statistics
Assuming a 50% efficacy of hydroxychloroquine in reducing the viral load at day 7, a 85%
power, a type I error rate of 5% and 10% loss to follow-up, we calculated that a total of 48
COVID-19 patients (ie, 24 cases in the hydroxychloroquine group and 24 in the control
group) would be required for the analysis (Fleiss with CC). Statistical differences were
evaluated by Pearson’s chi-square or Fisher’s exact tests as categorical variables, as
appropriate. Means of quantitative data were compared using Student’s t-test. Analyses were
performed in Stata version 14.2.
3. Results (detailed results are available in supplementary Table 1)
Demographics and clinical presentation
We enrolled 36 out of 42 patients meeting the inclusion criteria in this study that had at least
six days of follow-up at the time of the present analysis. A total of 26 patients received
hydroxychloroquine and 16 were control patients. Six hydroxychloroquine-treated patients
were lost in follow-up during the survey because of early cessation of treatment. Reasons are
as follows: three patients were transferred to intensive care unit, including one transferred on
day2 post-inclusion who was PCR-positive on day1, one transferred on day3 post-inclusion
who was PCR-positive on days1-2 and one transferred on day4 post-inclusion who was PCR-
positive on day1 and day3; one patient died on day3 post inclusion and was PCR-negative on
day2; one patient decided to leave the hospital on day3 post-inclusion and was PCR-negative
on days1-2; finally, one patient stopped the treatment on day3 post-inclusion because of
nausea and was PCR-positive on days1-2-3. The results presented here are therefore those of
36 patients (20 hydroxychloroquine-treated patients and 16 control patients). None of the
control patients was lost in follow-up. Basic demographics and clinical status are presented in
Table 1. Overall, 15 patients were male (41.7%), with a mean age of 45.1 years. The
proportion of asymptomatic patients was 16.7%, that of patients with URTI symptoms was
61.1% and that of patients with LRTI symptoms was 22.2%). All patients with LRTI
symptoms, had confirmed pneumonia by CTScan. Hydroxychloroquine-treated patients were
older than control patients (51.2 years vs. 37.3 years). No significant difference was observed
between hydroxychloroquine-treated patients and control patients with regard to gender,
clinical status and duration of symptoms prior to inclusion (Table 1). Among
hydroxychloroquine-treated patients six patients received azithromycin (500mg on day1
followed by 250mg per day, the next four days) to prevent bacterial super-infection under
daily electrocardiogram control. Clinical follow-up and occurrence of side-effects will be
described in a further paper at the end of the trial.
11
Hydroxychloroquine dosage
Mean hydroxychloroquine serum concentration was 0.46 μg/ml+0.2 (N=20).
Effect of hydroxychloroquine on viral load
The proportion of patients that had negative PCR results in nasopharyngeal samples
significantly differed between treated patients and controls at days 3-4-5 and 6 post-inclusion
(Table 2). At day6 post-inclusion, 70% of hydroxychloroquine-treated patients were
virologicaly cured comparing with 12.5% in the control group (p= 0.001).
When comparing the effect of hydroxychloroquine treatment as a single drug and the effect of
hydroxychloroquine and azithromyc in combination, the proportion of patients that had
negative PCR results in nasopharyngeal samples was significantly different between the two
groups at days 3-4-5 and 6 post-inclusion (Table 3). At day6 post-inclusion, 100% of patients
treated with hydroxychloroquine and azithromycin combination were virologicaly cured
comparing with 57.1% in patients treated with hydroxychloroquine only, and 12.5% in the
control group (p<0.001). These results are summarized in Figures 1 and 2. Drug effect was
significantly higher in patients with symptoms of URTI and LRTI, as compared to
asymptomatic patients with p<0.05 (data not show).
Of note, one patient who was still PCR-positive at day6-post inclusion under
hydroxychloroquine treatment only, received azithromycin in addition to hydroxychloroquine
at day8-post inclusion and cured her infection at day-9 post infection. In contrast, one of the
patients under hydroxychloroquine and azithromycin combination who tested negative at
day6 post-inclusion was tested positive at low titer at day8 post-inclusion.
Cultures
We could isolate SARS-CoV-2 in 19 out of 25 clinical samples from patients.
12
4. Discussion
For ethical reasons and because our first results are so significant and evident we decide to
share our findings with the medical community, given the urgent need for an effective drug
against SARS-CoV-2 in the current pandemic context.
We show here that hydroxychloroquine is efficient in clearing viral nasopharyngeal carriage
of SARS-CoV-2 in COVID-19 patients in only three to six days, in most patients. A
significant difference was observed between hydroxychloroquine-treated patients and controls
starting even on day3 post-inclusion. These results are of great importance because a recent
paper has shown that the mean duration of viral shedding in patients suffering from COVID-
19 in China was 20 days (even 37 days for the longest duration) [19]
Very recently, a Chinese team published results of a study demonstrating that chloroquine and
hydroxychloroquine inhibit SARS-CoV-2 in vitro with hydroxychloroquine
(EC50=0.72%μM) found to be more potent than chloroquine (EC50=5.47%μM) [14]. These
in vitro results corroborate our clinical results. The target values indicated in this paper [14]
were reached in our experiments. The safer dose-dependent toxicity profile of
hydroxychloroquine in humans, compared to that of chloroquine [13] allows using clinical
doses of hydroxychloroquine that will be over its EC50 observed in vitro [14].
Our preliminary results also suggest a synergistic effect of the combination of
hydroxychloroquine and azithromycin. Azithromycin has been shown to be active in vitro
against Zika and Ebola viruses [20-22] and to prevent severe respiratory tract infections when
administrated to patients suffering viral infection [23]. This finding should be further explored
to know whether a combination is more effective especially in severe cases. Speculated
potential risk of severe QT prolongation induced by the association of the two drugs has not
13
been established yet but should be considered. As for each treatment, the cost benefits of the
risk should be evaluated individually. Further studies on this combination are needed, since
such combination may both act as an antiviral therapy against SARS-CoV-2 and prevent
bacterial super-infections.
The cause of failure for hydroxychloroquine treatment should be investigated by testing the
isolated SARS-CoV-2 strains of the non-respondents and analyzing their genome, and by
analyzing the host factors that may be associated with the metabolism of hydroxychloroquine.
The existence of hydroxychloroquine failure in two patients (mother and son) is more
suggestive of the last mechanism of resistance.
Such results are promising and open the possibility of an international strategy to decision-
makers to fight this emerging viral infection in real-time even if other strategies and research
including vaccine development could be also effective, but only in the future. We therefore
recommend that COVID-19 patients be treated with hydroxychloroquine and azithromycin to
cure their infection and to limit the transmission of the virus to other people in order to curb
the spread of COVID-19 in the world. Further works are also warranted to determine if these
compounds could be useful as chemoprophylaxis to prevent the transmission of the virus,
especially for healthcare workers. Our study has some limitations including a small sample
size, limited long-term outcome follow-up, and dropout of six patients from the study,
however in the current context, we believe that our results should be shared with the scientific
community.
14
Titles for figures
Figure 1. Percentage of patients with PCR-positive nasopharyngeal samples from inclusion to
day6 post-inclusion in COVID-19 patients treated with hydroxychloroquine and in COVID-
19 control patients.
Figure 2. Percentage of patients with PCR-positive nasopharyngeal samples from inclusion to
day6 post-inclusion in COVID-19 patients treated with hydroxychloroquine only, in COVID-
19 patients treated with hydroxychloroquine and azithomycin combination, and in COVID-19
control patients.
Acknowledgements:
We thank Céline Boschi, Stéphanie Branger, Véronique Filosa, Géraldine Gonfier, Nadège
Palmero, Magali Richez and all the clinical, technical and paramedical staffs of the
hospitalization units and laboratories for their support in this difficult context.
Funding source
This work was supported by the French Government under the «
Investissements d’avenir » (Investments for the Future) program managed by the
Agence Nationale de la Recherche (ANR, fr: National Agency for Research),
(reference: Méditerranée Infection 10-IAHU-03)
References
[1] Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and
15
the challenges. Int J Antimicrob Agents. 2020 Feb 17:105924. doi:
10.1016/j.ijantimicag.2020.105924. [Epub ahead of print]
[2] Wang LS, Wang YR, Ye DW, Liu QQ. A review of the 2019 Novel Coronavirus
(COVID-19) based on current evidence”. Int J Antimicrob Agents. 2020 [Epub ahead of print]
[3] WHO Director-General’s opening remarks at the media briefing on COVID-19 – 11 March
2020. [https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-
the-media-briefing-on-covid-19—11-march-2020]
[4] Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus
disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the
Chinese Center for Disease Control and Prevention. JAMA. 2020 Feb 24. doi:
10.1001/jama.2020.2648. [Epub ahead of print]
[5] Santé Publique France. Infection au nouveau Coronavirus (SARS-CoV-2), COVID-19,
France et Monde [https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-
infections-respiratoires/infection-a-coronavirus/articles/infection-au-nouveau-coronavirus-
sars-cov-2-covid-19-france-et-monde]
[6] Colson P, Rolain JM, Raoult D. Chloroquine for the 2019 novel coronavirus SARS-CoV-
2. Int J Antimicrob Agents. 2020 Feb 15:105923. doi: 10.1016/j.ijantimicag.2020.105923.
[Epub ahead of print]
[7] Colson P, Rolain JM, Lagier JC, Brouqui P, Raoult D. Chloroquine and
hydroxychloroquine as available weapons to fight COVID-19. Int J Antimicrob Agents. 2020
[Epub ahead of print]
16
[8] Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine
effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res
2020;10-0282.
[9] Gao J, Tian Z, Yang X. Breakthrough: Chloroquine phosphate has shown apparent
efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci Trends
2020 Feb 19. doi: 10.5582/bst.2020.01047. [Epub ahead of print]
[10] Chinese Clinical Trial Registry. http://www.chictr.org.cn/
searchproj.aspx?title=%E6%B0%AF%E5%96%B9&offi
cialname=&subjectid=&secondaryid=&applier=&study
leader=ðicalcommitteesanction=&sponsor=&studya
ilment=&studyailmentcode=&studytype=0&studystage=
0&studydesign=0&minstudyexecutetime=&maxstudyexe
cutetime=&recruitmentstatus=0&gender=0&agreetosign
=&secsponsor=®no=®status=0&country=&prov
ince=&city=&institution=&institutionlevel=&measure=
&intercode=&sourceofspends=&createyear=0&isupload
rf=&whetherpublic=&btngo=btn&verifycode=&page=1.
[11] Multicenter collaboration group of Department of Science and Technology of
Guangdong Province and Health Commission of Guangdong Province for chloroquine in the
treatment of novel coronavirus pneumonia. Expert consensus on chloroquine phosphate for
the treatment of novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020 Mar
12;43(3):185-188. doi: 10.3760/cma.j.issn.1001-0939.2020.03.009.
17
[12] Biot C, Daher W, Chavain N, Fandeur T, Khalife J, Dive D, et al. Design and synthesis
of hydroxyferroquine derivatives with antimalarial and antiviral activities. J Med Chem
2006;49:2845-2849.
[13] Marmor MF, Kellner U, Lai TY, Melles RB, Mieler WF; American Academy of
Ophthalmology. Recommendations on Screening for Chloroquine and Hydroxychloroquine
Retinopathy (2016 Revision). Ophthalmology. 2016 Jun;123(6):1386-94. doi:
10.1016/j.ophtha.2016.01.058. Epub 2016 Mar 16.
[14] Yao X, Ye F, Zhang M, Cui C, Huang B, Niu P, et al. In Vitro Antiviral Activity and
Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe
Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 2020 Mar 9. pii:
ciaa237. doi: 10.1093/cid/ciaa237. [Epub ahead of print]
[15] Raoult D, Houpikian P, Tissot Dupont H, Riss JM, Arditi-Djiane J, Brouqui P. Treatment
of Q fever endocarditis: comparison of 2 regimens containing doxycycline and ofloxacin or
hydroxychloroquine. Arch Intern Med. 1999 Jan 25;159(2):167-73.
[16] Lagier JC, Raoult D. Whipple’s disease and Tropheryma whipplei infections: when to
suspect them and how to diagnose and treat them. Curr Opin Infect Dis. 2018 Dec;31(6):463-
470. doi: 10.1097/QCO.0000000000000489. [x] Expert consensus on chloroquine phosphate
for the treatment of novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi. 2020
Mar 12;43(3):185-188. doi: 10.3760/cma.j.issn.1001-0939.2020.03.009.
[17] Amrane S, Tissot-Dupont H, Doudier B, Eldin C, Hocquart M, Mailhe M et al. Rapid
viral diagnosis and ambulatory management of suspected COVID-19 cases presenting at the
infectious diseases referral hospital in Marseille, France, – January 31st to March 1st, 2020: A
respiratory virus snapshot. Travel Med Infect Dis. 2020 [Epub ahead of print].
18
[18] Armstrong N, Richez M, Raoult D, Chabriere E. Simultaneous UHPLC-UV analysis of
hydroxychloroquine, minocycline and doxycycline from serum samples for the therapeutic
drug monitoring of Q fever and Whipple’s disease. J. Chromatogr. B Analyt. Technol.
Biomed. Life Sci. 2017: 1060, 166-172.
[19] Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for
mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study.
Lancet. 2020 Mar 11. pii: S0140-6736(20)30566-3. doi: 10.1016/S0140-6736(20)30566-3.
[Epub ahead of print]
[20] Retallack H, Di Lullo E, Arias C, Knopp KA, Laurie MT, Sandoval-Espinosa C, et al.
Zika virus cell tropism in the developing human brain and inhibition by azithromycin. Proc
Natl Acad Sci U S A. 2016 Dec 13;113(50):14408-14413. Epub 2016 Nov 29.
[21] Madrid PB, Panchal RG, Warren TK, Shurtleff AC, Endsley AN, Green CE, Kolokoltsov
A, et al. Evaluation of Ebola Virus Inhibitors for Drug Repurposing. ACS Infect Dis. 2015 Jul
10;1(7):317-26. doi: 10.1021/acsinfecdis.5b00030. Epub 2015 May 11.
[22] Bosseboeuf E, Aubry M, Nhan T, de Pina, JJ, Rolain JM, Raoult D, et al. Azithromycin
inhibits the replication of Zika virus. J Antivirals Antiretrovirals. 2018 10(1):6-11. doi:
10.4172/1948-5964.1000173.
[23] Bacharier LB, Guilbert TW, Mauger DT, Boehmer S, Beigelman A, Fitzpatrick AM, et
al. Early administration of azithromycin and prevention of severe lower respiratory tract
illnesses in preschool children with a history of such illnesses: A randomized clinical trial.
JAMA. 2015 Nov 17;314(19):2034-2044. doi: 10.1001/jama.2015.13896.












 A Flourish chart
A Flourish chart